|
Vascular Rings and Slings
Anatomical description
Anomalies in aortic arch development are classified as vascular rings and slings, many which may cause compression of the airway and lead to stridor and/or respiratory distress. The development of the aortic arch follows a progression of growth and regression to create the definitive vascular system surrounding the heart (Keane, Table 54-1).
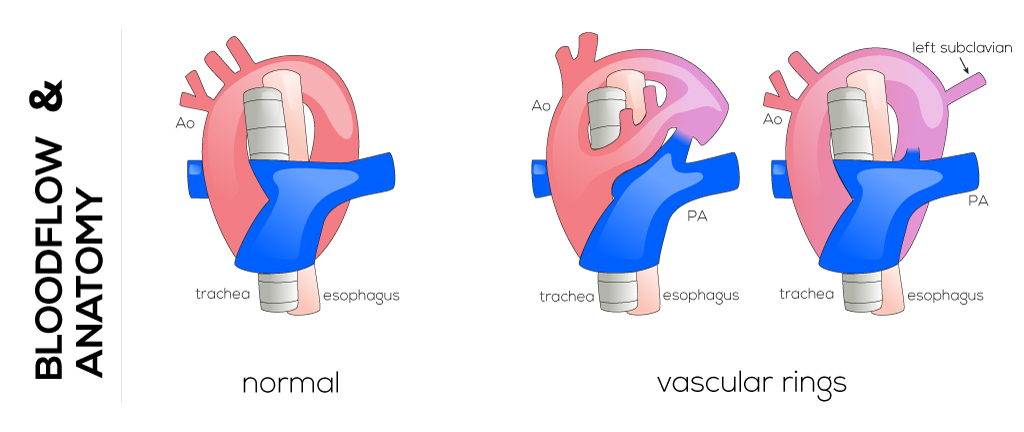
Vascular rings include defects in development of the aortic arch that leave the trachea and esophagus completely encircled by structures which are often fibrous, ligamentous remains of previously patent vessels. The most common types of vascular rings are the double aortic arch and right aortic arch with aberrant left subclavian artery. Together they comprise 90% of defects and usually exist as isolated congenital defects.
A double aortic arch results when both the right and left embryonic arches persist. They arise from the ascending aorta, pass around on both sides of the esophagus and trachea, then join at the posterior aspect to form the descending aorta. This arrangement creates a ring around the esophagus and trachea, usually partially composed of the ligamentum arteriosus (former ductus arteriosus). Each of the arches gives off a carotid and subclavian arch situated on either side of the trachea and esophagus.
A right aortic arch with aberrant left subclavian artery occurs as a result of regression in the aortic arch segment between the left common carotid and subclavian segments. This leaves the left subclavian arising as the last branch off the ascending aortic artery behind the esophagus. Typically, the esophagus and trachea are encircled and compressed by the ascending aorta and a ligamentum arteriosus that arises just distal and adjacent to the left subclavian artery.
Pathophysiology
Infants with a double aortic arch often present with stridor, dyspnea, and a barking cough, all which are due to tracheal compression. These symptoms worsen during feeding which may also trigger apnea that lasts seconds or minutes. In cases where a diagnosis is not made during infancy, this defect may be misdiagnosed as asthma and present in older children as a history of chronic cough or wheezing. Effects of esophageal compression are less common but include vomiting, choking, and difficulties in feeding.
The symptoms of a right aortic arch and aberrant left subclavian artery depend on whether the vascular ring is loose or tight. In cases where the ring is loose, patients may be asymptomatic and a diagnosis may be made only when imaging is performed for unrelated symptoms. In contrast, when the ring is tight, symptoms are identical to those in patients with a double aortic arch. Clinical manifestations of vascular rings can be traced to tracheal and esophageal compression.
Therapy
Surgical intervention is recommended for all patients with symptoms of tracheal or esophageal compression and is typically performed for those with a double aortic arch or right aortic arch with aberrant left subclavian when the encircling ring is tight. Almost all vascular rings are approached through a left thoracotomy with muscle-sparing technique and dissection of the posterior mediastinum. The surgical procedure involves a dividing of the ring to relieve compression of the structures, and thus respiratory and dysphagic symptoms. Further removal of the smaller portion of the double aortic arch or the division of the ligamentum arteriosus in children with right aortic arch and a vascular ring are required.
|