|
Congenitally "Corrected" Transposition of Great Arteries
Also called "Corrected" transposition of the great arteries, this refers to atrial-ventricular discordance and transposition of the great arteries (ventricular-arterial discordance).
Anatomical description
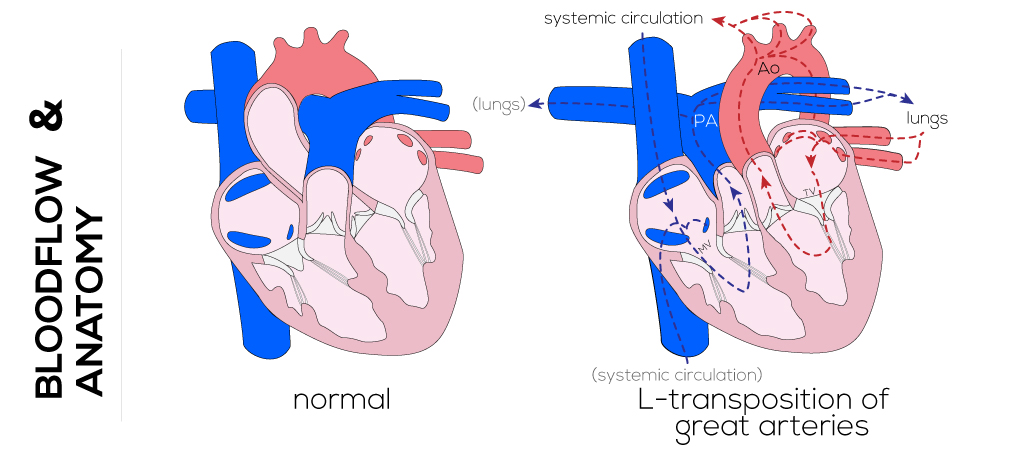
Desaturated systemic venous blood passes from the anatomic right atrium through a mitral valve into a morphologic right-sided left ventricle which has the pulmonary artery as an outlet. Pulmonary venous blood passes through the anatomic left atrium through a tricuspid valve into a morphologic left-sided right ventricle and out the aorta. Because the oxygen saturation of the arterial blood supply is normal, the defect is referred to as "corrected."
The lesion is one of two types: 1) the more common SLL, and 2) its mirror image, the IDD (less common). In this naming scheme, the first letter refers to the type of visceroatrial sinus, solitus (S), inversus (I), or ambiguous (A); the second letter to the type of ventricular sinus, D-loop ventricles with the right ventricle on right side and left ventricle on left side (D) or L-loop ventricles with the right ventricle on the left side and left ventricle on the right (L); and the third letter to the relationship of the great arteries, dextro being non-malpositioned with the aortic valve on the right side (D) or levo (L) with the aortic valve on the left side relative to the pulmonary artery.
SLL is characterized by situs solitus of the atria and viscera and levocardia. In this case, the superior and inferior vena cavae lie on the right side and drain into the right atrium. The right atrium empties into a finely trabeculated left ventricle through a mitral valve with two papillary muscles (L-looping). The great vessels are said to be inverted with the aortic valve to the left relative to the pulmonary valve and lie in a parallel rather than crossed position as in the normal anatomy.
Although SLL is more common than IDD, it is still considered a rare defect with an incidence of 0.02-0.07 per 1,000 live births. In the period between 1988 and 2002 at Children's Hospital in Boston, there were 83 patients diagnosed with SLL and 20 diagnosed with IDD. The IDD type is a mirror image of SLL and consists of situs inversus (inversion of the abdominal organs) and dextrocardia. In this case, the superior and inferior vena cavae are left-sided and drain into an atrium that opens to a left ventricle. The left ventricle then connects to a left-sided pulmonary artery. The right atrium receives the pulmonary venous return which then drains into a morphologic right ventricle through a tricuspid valve (D-loop). The right ventricle then connects to a right-sided anterior aorta (D transposition).
In most cases, these defects do not occur in isolation, but rather are accompanied by other cardiac anomalies. The most common associated problems include tricuspid valve problems (83%), VSDs (60%), pulmonary stenosis (59%), mitral valve diseases (54%), and/or ASDs (43%).
(Click picture to show/hide bloodflows)
Pathophysiology
The physiology of "corrected" transposition of the great vessels is related to the associated defects. Specifically, the right ventricle becomes the systemic pump but does not perform this function as well as the normal left systemic pump, due to geometric and morphologic differences. Tricuspid insufficiency and systemic ventricular dysfunction can occur.
Infants with this defect show clinical features that are related to associated abnormalities in cardiac anatomy. These abnormalities are highly variable. Possible complications shortly after birth include complete heart block, cyanosis, and/or congestive heart failure. Regurgitation through the tricuspid valve and atrioventricular conduction abnormalities are also common findings that are known to progress and contribute to decreased long-term survival.
Therapy
Management of patients with "corrected" transposition of the great arteries depends on the associated defects and their tendency to progress over time. It is generally recommended that patients who are asymptomatic or with minor structural problems be medically followed after diagnosis rather than undergo immediate operation. The current surgical approach aims to convert the left ventricle into the systemic pump and right ventricle into pulmonary pump. This is done by performing an atrial switch operation for venous return combined with a second procedure to properly connect the arterial supply, largely limited nowadays though. Oxygen-rich blood from the pulmonary artery is directed to the aorta via the right ventricle, whereas deoxygenated blood is guided from the vena cava to the pulmonary artery via the left ventricle.
|