|
(Click picture to show/hide bloodflows)
Pathophysiology
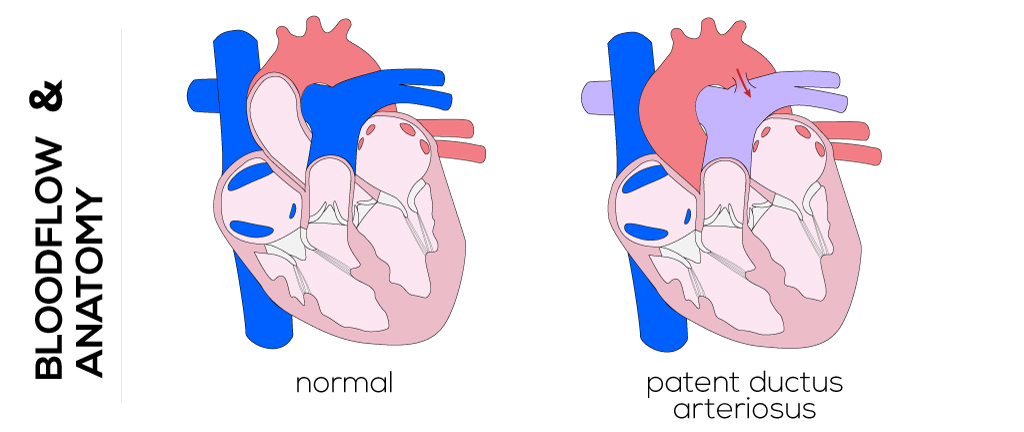
During fetal life, the ductus arteriosus connects the main pulmonary artery and aorta, carrying outflow from the right ventricle to the descending aorta and largely bypassing the lungs. Pulmonary resistance falls rapidly after birth when the infant takes its first breaths. Normally muscular constriction closes the ductus within a few hours. The lumen is then obliterated in a complex process requiring interactions between prostaglandins, changes in the level of arterial oxygen, genetics, and other unknown factors. This causes the patent tube of the ductus arteriosus to become a fibrous strand connecting the aorta and pulmonary trunk, referred to as the ligamentum arteriosus.
If the ductus arteriosus fails to close, the aortic and pulmonary arterial pressures equilibrate. This results in a decrease in pulmonary resistance which leads to left-to-right shunting and congestive heart failure. Excessive blood flow from the aorta to the pulmonary artery through a patent ductus leads to volume overload in the lungs, left atrium and ventricle, and ascending aorta. This may result in hypertrophy of structures, increased arterial pulse pressures, or pulmonary hypertension.
The clinical manifestations of patent ductus arteriosus vary depending on the size of the ductus and the amount of blood passing into the pulmonary circulation as a left-to-right shunt. A larger patent ductus arteriosus increases in size over the first months of life. It may be compensated with ventricular hypertrophy or remain even asymptomatic. A murmur is heard on auscultation and congestive heart failure with pulmonary hypertension can likely develop.
Therapy
The goal in management of patent ductus is to interrupt left-to-right shunting which, in turn, eliminates congestive heart failure, prevents pulmonary vascular disease and infective endocarditis, and promotes growth in infants of low birth weight. Medicinally, indomethacin and ibuprofen have been used to constrict the ductus and facilitate closure in premature infants. Surgical intervention is generally recommended for every patient with a patent ductus arteriosus that is not associated with other defects. Early surgical treatment has shown low operative morbidity and mortality rates.
In preterm children, a muscle-sparing fourth interspace posterolateral thoracotomy is performed to open the chest and the mediastinal pleura is opened longitudinally. Afterwards, the ductus is encircled and ligated. A multiple-suture ligation is particularly applicable to small infants. During the procedure, adequate ventilation must be maintained and hypothermia prevented.
In adults, the ductus is rather thin-walled and requires a different approach. A median sternotomy and cardiopulmonary bypass are administered. Occlusion is ensured by inverting the anterior wall of the pulmonary artery against the ductus.
Most isolated patent ductus arteriosus can be closed in the cardiac catheterization laboratory by coil embolization or other device methods.
|