|
Ebstein's Anomaly
Ebstein's anomaly is a rare defect that involves the tricuspid valve and right ventricle with an unknown embryology.
Anatomical description and types
There is significant variation in the anatomy of the valve but Ebstein's anomaly always involves, at least in part, the septal and posterior leaflets which are deformed and displaced toward the apex (downward), adherent to the ventricular septum. The wall of the right ventricle found near the adherent leaflets is said to be atrialized and very thin-walled. The right atrium is almost always enlarged, while enlargement of the right ventricle is more variable.
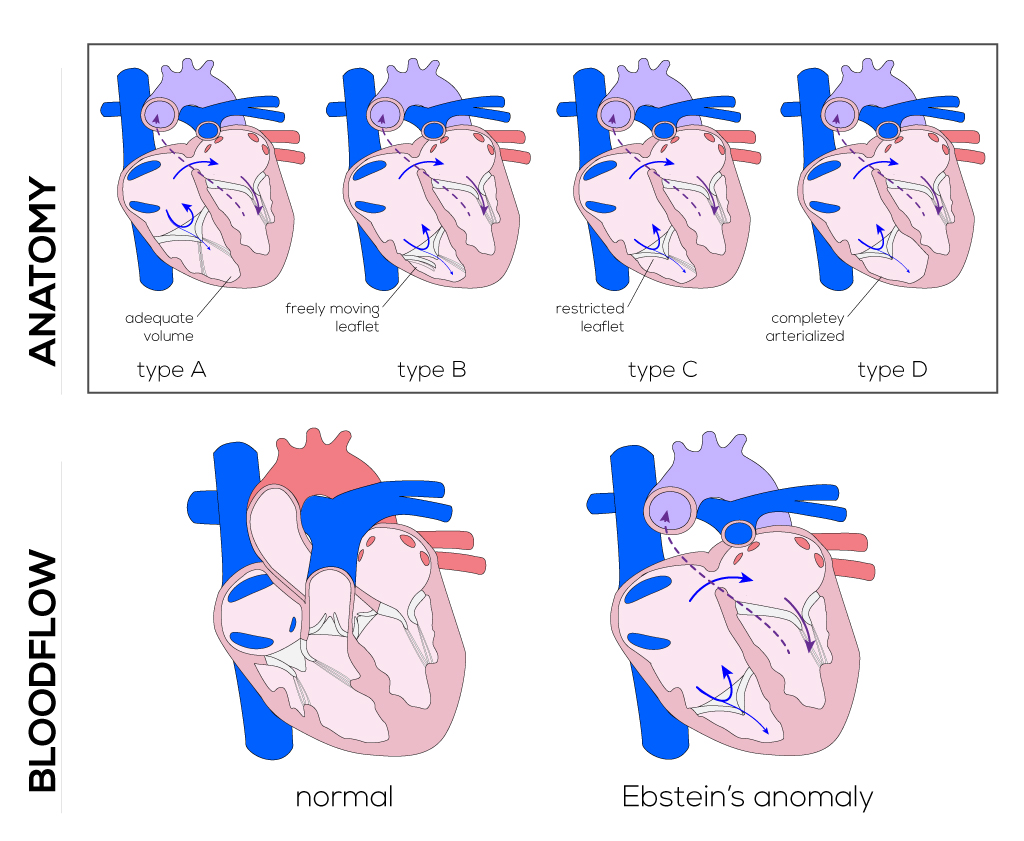
Four subtypes have been designated based on the relative volume of the right ventricle:
- Type A—right ventricle with adequate volume.
- Type B—large atrialized area of the right ventricle with freely moving anterior valve leaflet.
- Type C—anterior leaflet is highly restricted in movement and may obstruct the right ventricular outflow tract.
- Type D—ventricle is almost completely atrialized aside from a small infundibular portion.
Ebstein's anomaly is almost always associated with patent foramen ovale or ASDs. Other lesions including Tetralogy of Fallot, VSD, pulmonary stenosis, and pulmonary atresia may occur but are less common.
(Click picture to show/hide bloodflows)
Pathophysiology
Tricuspid insufficiency or stenosis and right ventricular impairment limit blood flow through the right heart and into the pulmonary artery. Increased right atrial pressure due to limited outflow leads to right-to-left shunting through the patent foramen ovale. This shunting causes a variable degree of cyanosis and cardiomegaly which is present at birth and is sometimes accompanied by tachypnea. Both pulmonary arterial resistance and right-to-left shunting decrease in the days and weeks after birth which may lessen the cyanosis initially present in infancy. With severe insufficiency of the tricuspid valve, the right ventricle might not generate pressures high enough to open the pulmonary valve, thus causing functional atresia and ductal dependency.
Therapy
During infancy, Ebstein's anomaly is typically managed by administering prostaglandins and/or nitrous oxide to increase pulmonary blood flow and control cyanosis. Complex surgical procedures may be performed to correct lesions, but long-term outcomes in controlled studies have yielded mixed results (Keane). Older children with Ebstein's anomaly are generally followed medically with special attention to rhythm abnormalities and congestive heart failure. Surgery is performed only on patients who are very symptomatic, cyanotic, or in congestive heart failure.
During infancy, a Blalock-Taussing shunt can be applied to insure pulmonary blood flow. This shunt is constructed by interposing a graft between the subclavian artery and the right or left pulmonary artery. Originally performed through a right/left thoracotomy, depending on the neonate’s anatomy, the procedure is nowadays usually completed through a median sternotomy. It allows for a shorter shunt which can be placed more centrally. Older patients undergo reparative procedures of the tricuspid valve or replacement procedures. Those techniques aim to reduce the size of the annulus of the tricuspid valve and utilize functional tissue to build a competent valve.
Procedures include: median sternotomy, cannulation, cardiopulmonary bypass, cardioplegia, and hypothermia. The right atrium will be opened after inspection of the coronary vasculature. For the Carpentier technique the anterior leaflet is mobilized first. Afterwards vertical plication sutures will be applied under consideration of a satisfactory anterior leaflet reconstruction. The leaflet will then be advanced across the plicated area to reduce the size of the valve orifice. Finally, an annular ring can be sutured in to support the tricuspid valve.
|












