|
This tutorial will teach you about the four main types of bifurcation stenting techniques. Please also see the general description of stents in the Device Tutorial page.
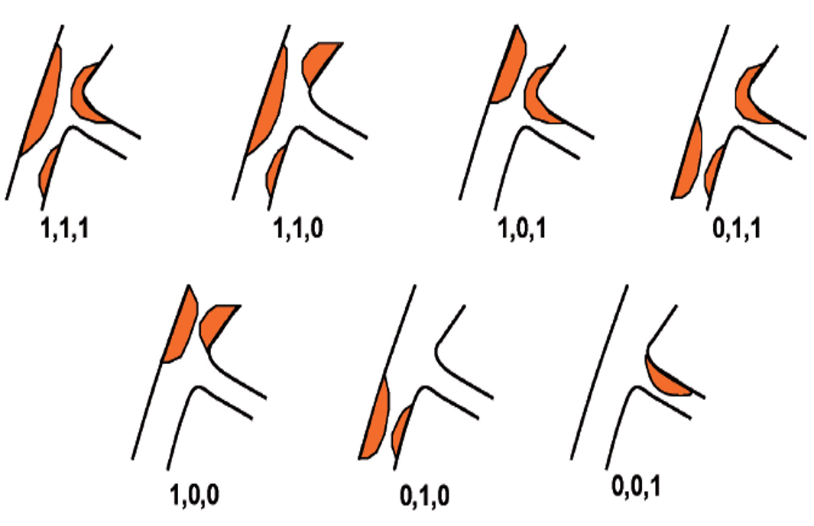
Depositions of plaque in the coronary artery vessels vary greatly from person to person, and some occlusions may be located bifurcations of the coronaries. A classification system known as the Medina system2 has become widely accepted and is recommended because it is considered a simple and effective way to describe bifurcation lesions. However, it has its limitations as it cannot be used to describe specific bifurcation angles, degrees of calcification and/or length of plaque involvement. In bifurcation lesions like these, treatment may only be possible by placing stents in both the main vessel and the side branch. Due to the specificity of every patient's coronary anatomy, it is extremely difficult to construct a "one-size-fits-most" bifurcation stent. Because of this, interventional cardiologists typically must manipulate one or more single vessel stents to conform them to a bifurcation. Every year, an elite group of bifurcation specialists known as the European Bifurcation Club (EBC) meet to discuss the most recent recommendations regarding bifurcation stenting. Each year is finalized by the development of a consensus3, in which the opinions, ideas and statements regarding bifurcation management are summarized.
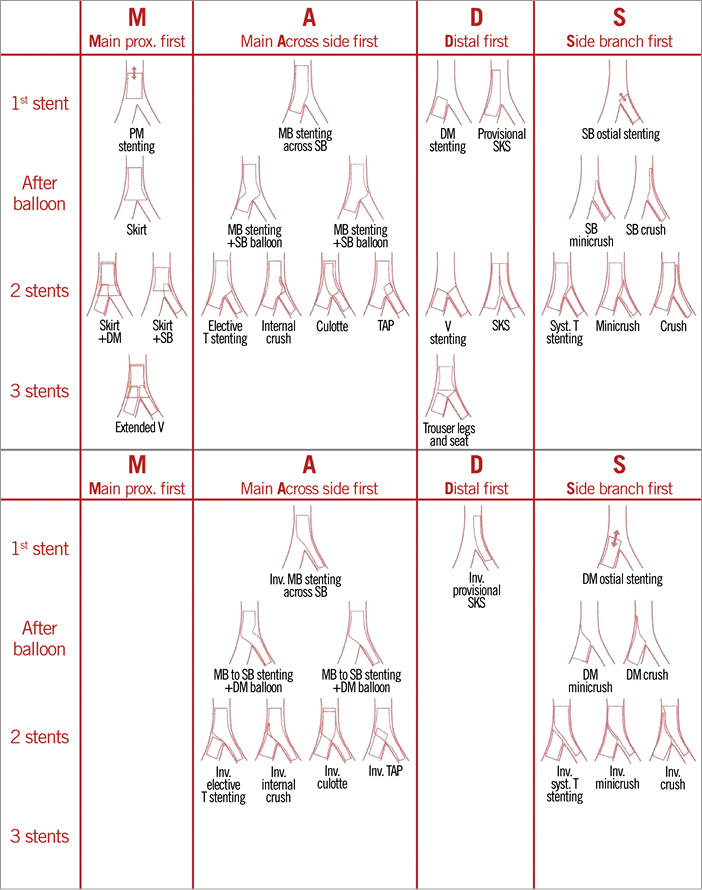
Under the pulldown menus provided in this tutorial, the reader will find several techniques, observed using the Visible Heart® methodologies4, that are designed to keep both the main and side branch vessels patent. Each technique varies by the order of operations taken as well as where the procedure starts and ends. The MADS classification5 was developed as a decision-making tree to be coupled with the Medina system to offer better patient care. Using the Medina classification system, an interventional cardiologist can classify plaque deposition and follow up with MADS to narrow down which technique is best to treat the individual patient. As shown in the image below, each bifurcation technique is comprised of a series of steps; current recommendations are described in detail below.
Stent Deployment
Using fluoroscopy as the main imaging modality, guidewires are placed so that there is at least one wire down each of the bifurcation vessels. Once the wires are positioned, a stent can be fed along the wires and placed in the corresponding vessel. Upon proper positioning, a given stent is then inflated to a high pressure (12 atm or more) to expand the stent within the lumen. This is just the beginning of bifurcation techniques, as additional measures are needed to ensure proper apposition and to ensure that flows through side branches are not obstructed, reducing the risk of restenosis or adverse healing (e.g., malapposition or delayed endothelialization) over time.

Rewire
After deployment of an initial stent, regardless of which branch, there are two needs that must be addressed: flow into the opposite branch may be compromised and the secondary guidewire has been jailed. In these cases, the guidewire from the main branch is carefully withdrawn and fed through the stent struts and into the side branch if possible. The jailed wire is then pulled back proximally to the stent and rewired through the main branch. After successful rewiring, additional steps can be taken to perform various bifurcation techniques, e.g. a kissing balloon technique or a POT.
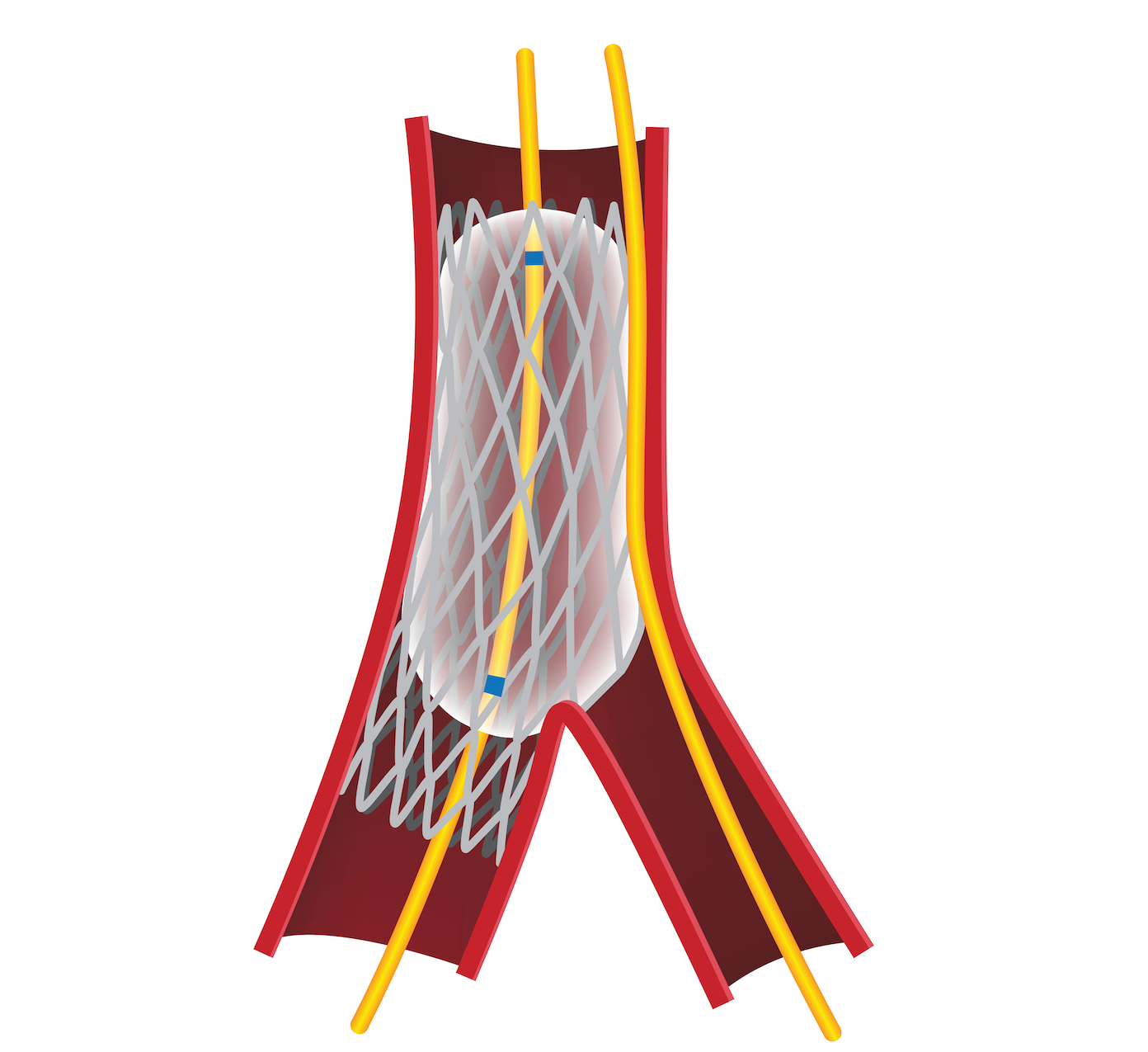
Proximal Optimization Technique (POT)
The proximal optimization technique (POT) is a methodology to improve the end results of stent scaffolding for treating bifurcation lesions. Stents are typically sized to the end diameter of the distal vessel, which means that the proximal end of the stent is initially undersized relative to the vessel diameter due to vessel taper. This discrepancy can create issues with further stenting steps and increase the risk of malapposition and stent thrombosis. The POT step helps remove this risk. An appropriately sized balloon is inflated in the main vessel just proximal to the carina, defined as the ridge of the vessel that splits the vessel into its bifurcations. When performed properly, the technique improves stent apposition in the proximal main vessel and also facilitates side branch access after main vessel stent implantation.
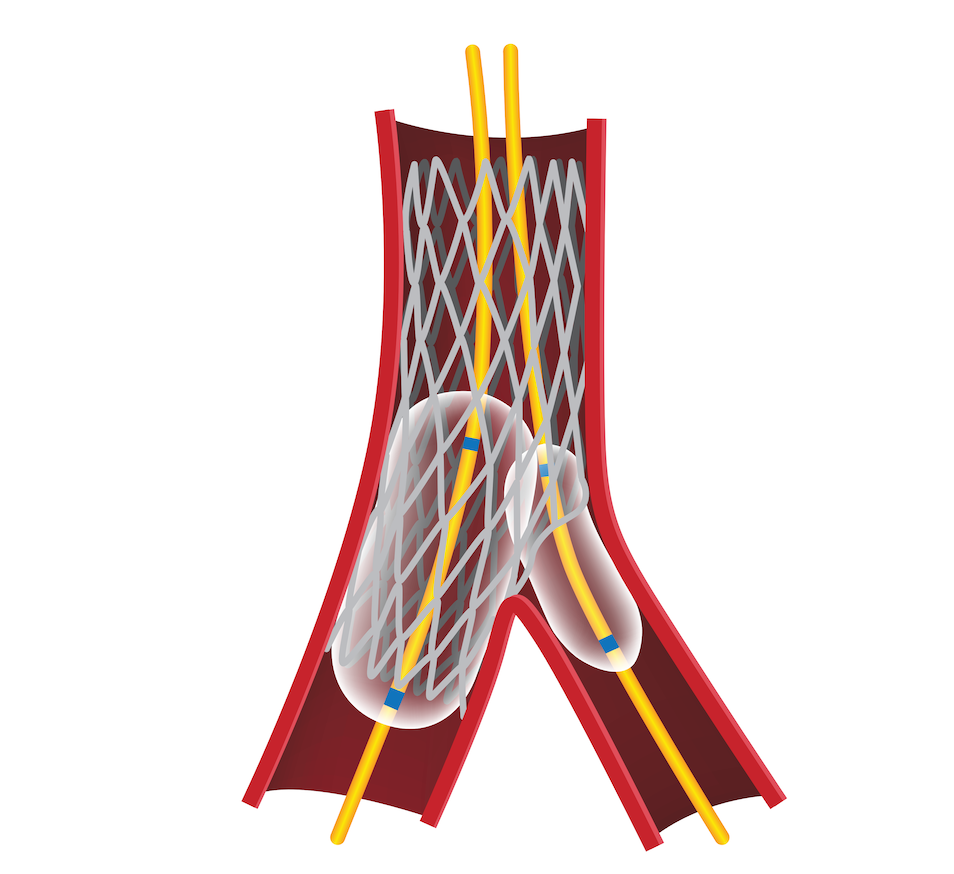
Kissing Balloon Technique (KBT)
A kissing balloon technique (KBT) is a strategy used to properly apposition the stents along the bifurcation while maintaining the native position of the carina.This technique is typically performed as an intermediary step during bifurcation stenting, following main vessel stent deployment and rewiring of the side branch. Guidewires are positioned in both the main and side branches, with one or two stents already deployed, depending on the chosen bifurcation strategy. Two properly sized balloons are fed down the guidewires and placed so that the balloons overlap with the carina. Once positioned, both balloons are inflated to the same pressures and simultaneously deflated to ensure that the carina is not shifted into either one or the other side of the given bifurcation.
References:
- Lloyd-Jones, D., Adams, R. J., Brown, T. M., Carnethon, M., Dai, S., De Simone, G., ... & Go, A. (2010). Heart disease and stroke statistics--2010 update: a report from the American Heart Association. Circulation, 121(7), e46.
- Stankovic G, MD, PhD., et al. "Percutaneous coronary intervention for bifurcation lesions:2008 consensus document from the fourth meeting of theEuropean Bifurcation Club" EuroIntervention. 2009;5:39-49.
- Adrian P. Banning, MD; Jens Flensted Lassen, MD; Francesco Burzotta MD, PhD et al. "Percutaneous coronary intervention for obstructive bifurcation lesions: the 14th consensus document from the European Bifurcation Club". EuroIntervention 2019;15:90-98. DOI: 10.4244/EIJ-D-19-00144
- Burzotta F, MD, PhD., Cook B, PhD, Iaizzo PA, PhD, Singh J, PhD, Louvard Y, PhD, Latib A, MD, PhD. "Coronary bifurcations as you have never seen them: the Visible Heart® Laboratory bifurcation programme." EuroIntervention 2015
- Jens Flensted Lassen MD, PhD et al., "Percutaneous coronary intervention for coronary bifurcation disease: consensus from the first 10 years of the European Bifurcation Club meetings". EuroIntervention 2014;10:545-560
- DeVos A, PhD, Reifart J, MD, Valenzuela T, Phd, et al. "Percutaneous Coronary Intervention: Devices, Research, and Clinical Implications." Handbook of Cardiac Anatomy, Physiology, and Devices," 4th edition, edited by Paul Iaizzo, PhD., Springer, 2024, pp.805-833.
|



