University of Minnesota
http://www.umn.edu/
612-625-5000
Atrial septal defects (ASDs)
Atrial septal defects are characterized by deficiencies within the atrial septum. These defects can range from a single hole in the fossa ovale to multiple small fenestrations.
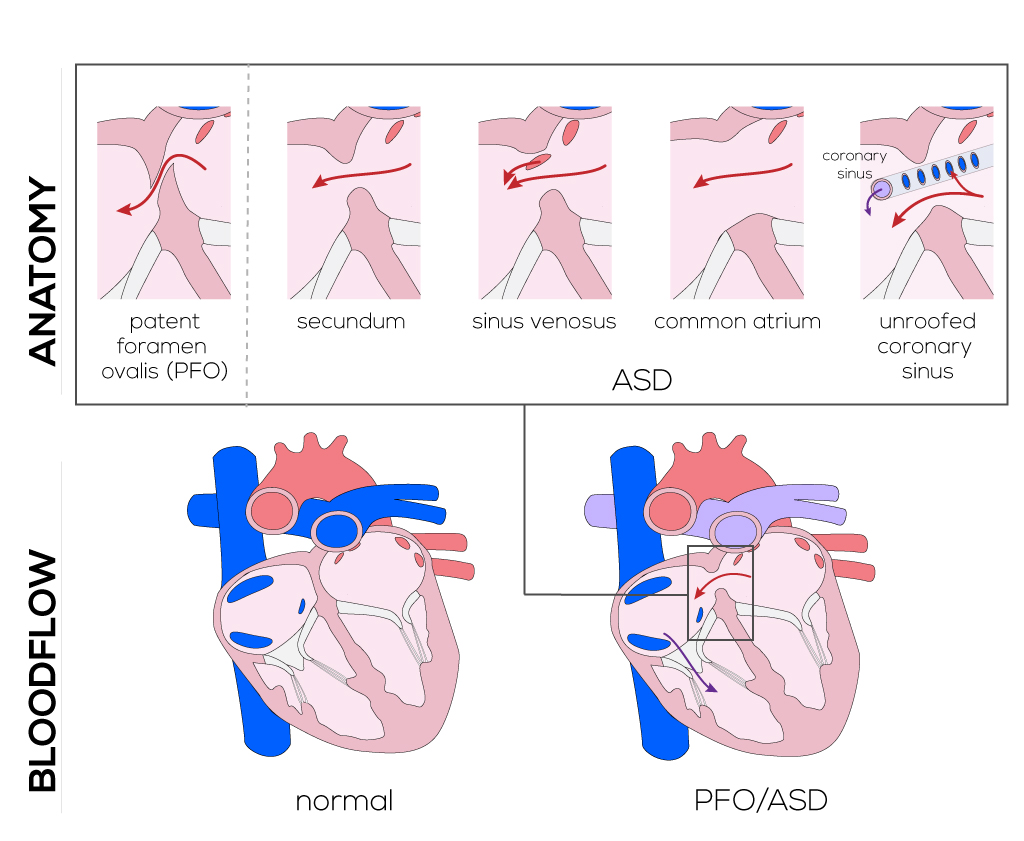
Anatomical description and types
Patent foramen ovale—persistent atrial communication past the fetal period due to incomplete closure of the foramen after birth.
Secundum atrial septum defect—defect in the septum primum (most common).
Sinus venosus atrial septal defect (superior and inferior)—involves the septum secundum near the superior vena cava or coronary sinus (infrequent). These defects are most often associated with partial anomalous pulmonary venous return.
Common atrium—absence of the septum primum, septum secundum, and septum of the atrioventricular canal. This defect is typically associated with “Heterotaxy Syndrome.”
Unroofed coronary sinus—defective formation in all or parts of the atrial wall separating the left atrium and coronary sinus. These defects can be strongly associated with the presence of a left superior vena cava, which is known as “Raghib Syndrome.” In this case, the left superior vena cava drains into the superior aspect of the left atrium, often communicating with the coronary sinus.
An atrial septal defect is observed here. This opening allows blood to flow between the left and right atria, and facilitates the mixing of oxygenated and deoxygenated blood.
(Click picture to show/hide bloodflows)
Clinical presentation
Typically, these patients are diagnosed in early childhood by a pediatrician versus family physicians. If these patients with moderate to large ASDs are undiagnosed can result in a fixed pulmonary vascular disease in adulthood. These patients may not be a candidate for surgical versus catheter based intervention because they have developed Eisenmenger’s syndrome (fixed pulmonary bed shunting right to left). Patient will be cyanotic, decreased exercise tolerance, stroke.
Pathophysiology
Atrial septal defects allow blood to shunt from the left atrium to the right atrium. Shunting is minimal during infancy, but typically increases with age as the right ventricle becomes more compliant.
Most infants are asymptomatic but may develop congestive heart failure or elicit growth failure if the left-to-right shunt is significant. In these cases, the infants often have additional heart defects as well as extracardiac anomalies, which may contribute to their overall slowed growth. Older adults may develop right atrial and ventricular dilatation, congestive heart failure, atrial fibrillation, and rarely pulmonary vascular obstructive disease. Right ventricular dilatation can cause tricuspid insufficiency. Pulmonary congestion and hypertension can occur with large shunts. Results are right-to-left shunting and cyanosis in untreated older patients, which create a risk for systemic emboli and stroke.
Therapy
It is recommended that atrial septal defects 8mm or larger with presence of a left-to-right shunt be closed upon identification in order to prevent pulmonary vascular disease or arrhythmias. Smaller defects, particularly those less than 3mm, often close spontaneously.
One-year-old male, asymptomatic, presents to the pediatrician for routine physical exam and was noted to have a heart murmur. He has normal growth and development. This patient was referred to the pediatric cardiologist for further evaluation, which includes physical exam, ecg and echocardiogram. The physical exam showed normal S1, fixed S2, systolic murmur grade 2 out of 6 in the left upper sternal border. ECG shows normal ventricular rate, rSR', normal ventricular forces. The video demonstrates an Transesophegeal echo (TEE) of a moderate to large secundum ASD and right heart enlargement, first showing basic anatomical description, then highlighting the ASD, next highlighting the enlarged right heart. The video then demonstrates the transcatheter ASD closure with Amplatz septal occluder.
Cardiac catheterization is a procedure which is used to repair secundum defects. A catheter is inserted into a vessel in the groin and guided to the heart. Through the catheter, a patch can be inserted into the hole. Tissue growing around the patch will permanently close the defect.
Open-heart surgery is another method used for large secundum type defects as well as primum, sinus venosus, and coronary sinus types. This procedure requires either a sternotomy or a right thoracotomy; the latter is preferred for cosmetic reasons. Anesthesia and a cardiopulmonary bypass are instituted, and cannulas are placed in the aorta, in addition to the superior and inferior vena cava. To prevent air embolism, since the left heart is open to the atmosphere through the ASD, the ascending aorta is clamped until the defect is repaired and all air has been removed from the heart. A systemic hypothermia of approximately 28°C and cardioplegia are used to protect the myocardium.
The right atrium is opened by a longitudinal incision from the appendage to the inferior vena cava. The area of the sinoatrial node and crista terminalis are avoided to prevent postoperative supraventricular tachycardia. The usual procedure for secundum defect closure is a knitted patch secured with nonabsorbable sutures. The option of a direct closure is only applied when tension is minimal, but it also has a higher risk of recurrence.
The patch technique is always used for closure of sinus venosus defects because of its anatomical location at the junction of the superior vena cava and right atrium. This is applicable for ostium primum ASDs in order to avoid tension. During this procedure, the cleft in the anterior mitral leaflet is sutured while additional sutures around the annulus are used to secure cleft edges. Next, the patch is sutured to the leaflet tissue that bridges the crest of the ventricular septum between the mitral and tricuspid valves. After the patch is attached successfully, air from the left side of the heart can be released through a vent and the aorta can be unclamped. Normally the heart spontaneously starts beating in a normal sinus rhythm, otherwise the patient is defibrillated before left ventricular vent removal. Bypass connection is removed and the incisions are closed via sutures.
Comparing nonsurgical and surgical closure procedures, statistics show no significant difference in success rate. Rather it suggests a lower complication rate and a shorter hospitalization for device closure than surgical intervention. Appropriate patient selection is the most important factor in ensuring positive results using catheterization methods.