|
Aortopulmonary Window (APW) Defects
Aortopulmonary window defects are rare and result from a failure in development of the endocardial cushion tissues in the fetal common outflow tract.
Anatomical description and types
Without proper fusion between the opposing cushion tissues, there is incomplete septation between the ascending aorta and main pulmonary artery. Consequently, there are typically two distinct semilunar valves present at the proximal end of both the aorta and pulmonary trunk.
Defects can be classified by their relative locations:
- Type I defects are located just above the semilunar valves (most common).
- Type II defects exist in the most distal aspect of the ascending aorta.
- Type III defects encompass both the proximal and more distal areas of the ascending aortic and pulmonary vessels.
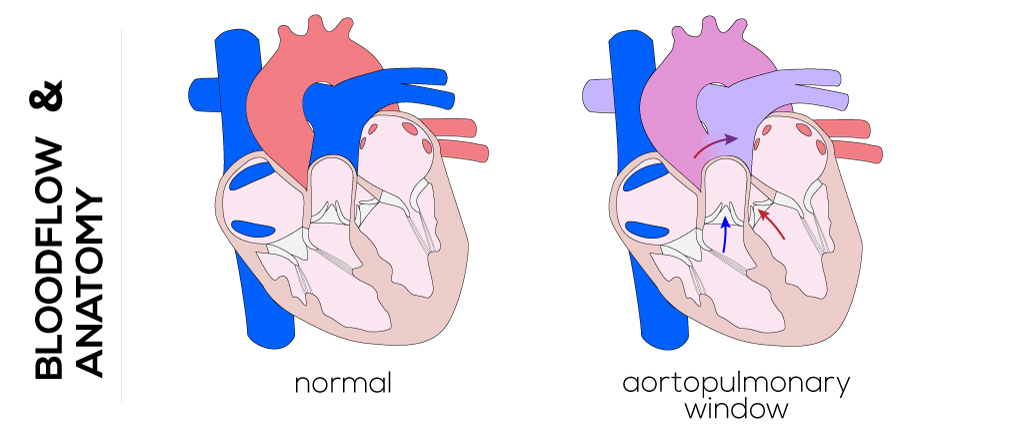
(Click picture to show/hide bloodflows)
Pathophysiology
AWDs present with similar physiological features as patent ductus arteriosus or ventricular septum defects. They result in a left-to-right shunt which typically leads to early pulmonary hypertension and congestive heart failure, depending on the size of the window which is commonly large. Pulmonary vascular disease typically develops when the window is not surgically repaired.
Therapy
Surgical closure and repair of associated lesions are recommended to be performed soon after diagnosis in order to survive infancy and decrease the risk of pulmonary vascular diseases.
A median sternotomy is usually performed followed by cardiopulmonary bypass. Meanwhile the pulmonary arteries are controlled and occluded. The aortic cannula must be far away from the defect to not interfere with the repair. Cardioplegia with moderate hypothermic arrest or deep hypothermic circulatory arrest in small children is utilized. Most defects require a closure patch, either one- or two-patch technique, whereas the coronary ostia must be included at the aortic side of the patch. The APW is opened anteriorly after cross-clamping and, under consideration of the anatomical structures, closed with one or two patches to prevent stenosis.
|












