|
Congenital Heart Defects
|
There are numerous congenital defects in human hearts and many typically require medical intervention. Inportantly, congenital defects of the human heart present a unique challenge in establishing an accurate and consistent nomenclature that is secondary to our somewhat incomplete understanding of their embryologic origin and vast complexity of varied anatomic presentation (1). In any attempt to describe a complex system, several lines of reasoning may evolve that foster not only controversy but also confusion. An adequate system to describe congenital lesions of the human heart is no exception. Nevertheless, several leading clinicians and investigators in this field can be credited with the primary elucidation of a system that attempts to organize and categorize these complex lesions (1).
In the 1970's, Richard Van Praagh presented a system based on the segmental anatomy of the developing heart (2,3). His generalized theory states that, by understanding the anatomical position of the cardiac segments, the majority of cardiac defects may be accurately described. The three segments which Van Praagh described consist of the atria, the ventricle, and the great vessels. These segments may be described by delineating their relative positional relationships. The visceroatrial situs is defined as the relative position of the right and left atria to the sidedness of the abdominal (visceral) organs; the term situs means position or location. The bulb ventricular loop is described as the orientation of the right and left ventricles to the great vessels (pulmonary artery and aorta). These segments are referenced in sequence, with each being designated by a letter. The connection of the visceral venous vessels (the superior and inferior vena cavae) and the atrial body is termed the visceroatrial situs and is described by the letters: S, Situs Solitus; I, Situs Inversus; and A, Situs Ambiguous. When the visceral situs is normal (Situs Solitus), the stomach and spleen lie to the left, the right lobe of the liver is larger than the left, and the appendix is right-sided. In Situs Inversus, the position of the abdominal organs is reversed, with the stomach and spleen lying on the right and the dominant lobe of the liver to the left; the appendix and inferior vena cava are to the left, with the left lung being typically trilobed. Situs Ambiguous describes a group of anomalies in which the dominant characteristic is a lack of visceral sidedness. The abdominal organs may be positioned to the anatomic left or right, often with the liver lying in the midline. A unique characteristic of these individuals is the abnormal existence or a complete lack of a spleen. In general, polysplenic patients tend to have all atrial and pulmonary structures consistent with left-sided morphology, while asplenic patients tend to be right-sided dominant (4). These various defect will be specifically described in various sections of this tutorial.
|
|
|
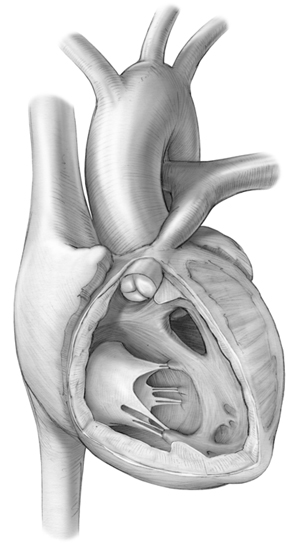
Four components of Tetralogy of Fallot include:
pulmonary annular hypoplasia, a malaligned ventricular septal defect,
right ventricular hypertrophy, and an overriding aortic annulus. The
defect is viewed by removal of the right ventricular free wall (1).
|
|
Additionally, the orientation of the right or left ventricular mass is described by how the embryonic cardiac tube loops during its development. In this system, the terms "right" and "left" are used to refer to the specific morphology of the ventricular mass rather than their spatial arrangement. The anatomic right ventricle has a very trabeculated endocardium, while the left ventricular endocardium is smooth with finer trabeculation. The rightward (normal) orientation is given the term "D" for D-loop. This indicates that the morphologic right ventricle is oriented to the right and anterior to the morphologic left ventricle. If the cardiac tube undergoes looping in the leftward direction, the segment is given the reference letter "L" for L-looping. In this situation, the morphologic right ventricle lies posterior and to the left of the morphologic left ventricle. The final segmental orientation described by Van Praagh deals with the relationship of the great vessels and semilunar valves to the ventricles. The aorta is normally committed to the morphologic left ventricle with the aortic valve located leftward and posterior to the pulmonary valve. This normal relationship is given the reference letter "S." When the great vessels are transposed, with the aortic valve being rightward and anterior to the pulmonary valve, the convention used is "D." With D-transposed great vessels, the aorta is committed to the morphologic right ventricle and the pulmonary artery and valve to the morphologic left ventricle. When the orientation of these great vessels and semilunar valves are normal, but the aorta is committed to the right ventricle and the pulmonary artery to the left ventricle, the term L-transposed great vessels is used.
- St. Louis, JD. Congenital Defects of the Human Heart: Nomenclature and Anatomy. Chapter 9, Handbook of Cardiac Anatomy, Physiology, and Devices. Iaizzo PA (Editor), Springer pp. 137-144, 2009.
- Van Praagh R. Terminology of congenital heart disease: Glossary and commentary. Circulation 1977;56:139
- Van Praagh R, Vlad P. Dextrocardia, mesocardia, and levocardia: The segmental approach in congenital Heart disease. In: Keith JD, Rowe RD, Vlad P, eds. Heart disease in infancy and childhood. 3rd ed. New York, NY: Macmillian, 1978
- Seo JW, Brown NA, Ho SY, Anderson RH. Abnormal laterality and congenital cardiac anomalies. Relations of visceral and cardiac morphologies in the mouse. Circulation 1992;86:642-50
|



